- Home
 Care Partner
Care Partner-
Software
-
Service User Records
Service User Records
This section covers the key features of the service user record and provides guidance on maintaining the service user record.
Personal Details (including Other Personal Details)
Accessing the Service User Record
You can access a service user’s record from wherever you see a service user name displayed in Care Partner.
Service User Record
By default the Summary screen of the service user record will be displayed when the record is accessed.
The Summary screen provides access to key information about a service user in a single click. The information on this screen pulls from the relevant sections of the record.
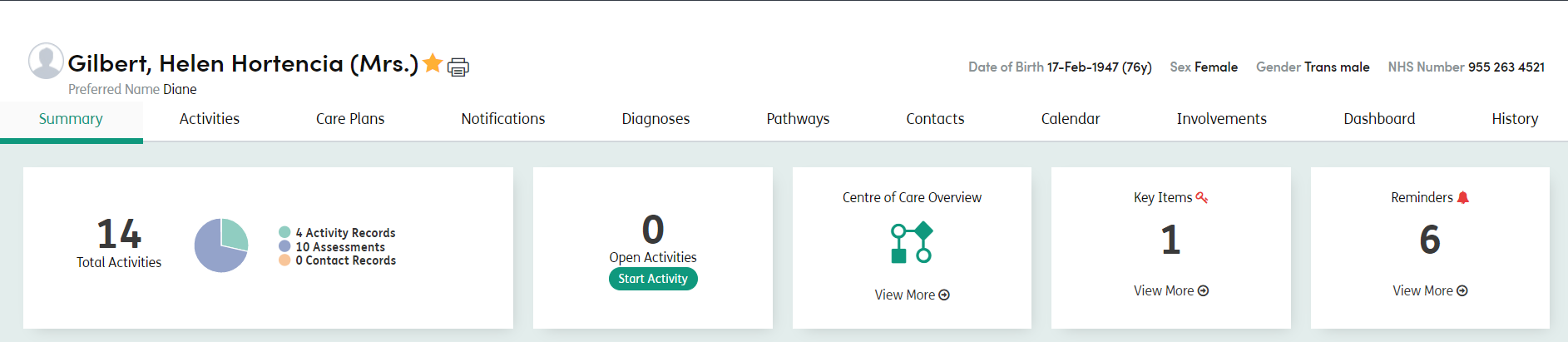
The tabs immediately below the patient’s name will help you to navigate between the different sections of their record:
Summary: Key information pulled from all the different sections is displayed here.
Activities: Within Care Partner, an Activity can be either an Assessment (for example, a Risk Assessment) or a record of an intervention with a Service User (for example, a Contact Record). This section allows you to record a new activity or view and edit existing activities.
Care Plans: Records the service user’s needs, goals and outcomes and the interventions needed. It also records the Contact Records linked to the Plan.
Notifications: Key information about a service user that all staff members need to be aware of, for example a risk or an allergy. This includes Alerts, Key Items and Reminders.
Diagnosis: Record Primary, Unrelated, Related and Provisional Diagnoses.
Pathways: Record the service user’s pathways
Contacts: Information for both Professional and Personal Contacts.
Calendar: Allows users to add and view events for service users, as well as recording attendance.
Involvements: Information about which Centres of Care the service user belongs to, both current and historical.
Dashboard: An overview of Service User’s data and Key Item Reports.
History: A basic history of what staff and users have changed, updated or viewed in the service user’s record.